(Editor Note: Insight Bytes focus on key economic issues and solutions for all of us, on Thursdays we spotlight in more depth Solutions to issues we have identified. Fridays we focus on how to build the Common Good. Please right click on images to see them larger in a separate tab.)

Photo: healtheconomics.com
Several states including New York, Vermont, Massachusetts and California have begun initiatives to take on drug companies for the their exorbitant prices of new drugs. New York is taking a price versus effectiveness approach with a new drug called Orkambi for cystic fibrosis. The New York state Medicaid department is demanding a lower price as it is not clear the drug helps patients with the disease better than existing treatments. Vertex, the manufacturer of Orkambi made $1.3 billion in sales from the drug which is a high sales level for a drug that is marketed to only 26,000 eligible patients. Vertex prices Orkambi at $272,000 for one year of doses. The drug costs so much that some insurers pass on the high costs to patients in some cases $3000 per month.
Dr. Steven D. Pearson, President of the Institute for Clinical and Economic Review is working with New York officials on a state board case against Vertex to bring the price down. The state board found that Orkambi did not meet the effectiveness claims by the manufacturer so New York should receive a 77 % discount. Dr. Pearson said his evaluation of the costs indicated that the drug could be discounted by 77 %.
Major states like New York and California are taking on the drug companies with renewed interest as their Medicaid costs soar in part from new drugs where companies like Vertex price the medication at extreme multiples of a fair cost. While the GOP Administration has promoted some ideas to bring the cost of new drugs down, nothing to date has been done.
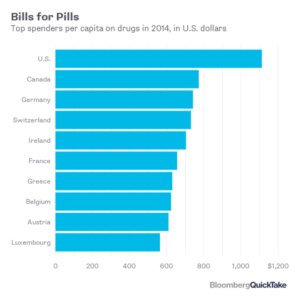
The U.S. is alone of all major developed countries in not directly regulating drug prices. In Europe health services officials do not accept high prices for drug with marginal value and negotiate using their purchasing power to bring the price down. Congress has consistently bowed to the drug lobby by not speeding generic drugs to the market and not including in any drug bill the power for Health and Human Services to directly negotiate the price of all the medications it covers for U.S. patients.
Source: Bloomberg – 5/11/18
In 2014, U.S. patients paid the most of ten developed countries at $1,100 per year out of pocket and for many patients with difficult treatment diseases the costs per year are significantly more.
Next Steps:
Time is up for the drug companies and insurers gouging patients with soaring prices while they make hefty profits and executives pocket huge compensation packages. Drug companies need to stop buying back their stock, wasting the money that could be used to bring the price of their drugs by billions of dollars. Congress needs to give HHS the power to negotiate prices and effectiveness limits on drugs of dubious value the way most developed countries in the world do today. Over the past decade pharmaceutical companies have found that their exorbitant prices have not stuck in Europe or other developed country market, so they jack up the price of the medication in the U.S. where there is little regulatory constraint.